
In this article, I’m interviewing Salu Ribeiro, the co-founder and CEO of Bay Area Phlebotomy and Laboratory Services, a CLIA-certified laboratory and sample transportation, processing, and test distribution service based in the San Francisco Bay Area. We’ll be talking about the basics on how IVF works. Salu graduated with a Bachelor of Science from the University of California at Davis and holds a Master of Science with Merit degree in clinical embryology and andrology from the University of Leeds in the United Kingdom.
Salu shares his expertise on everything from egg retrieval to embryo development, explaining what happens in the lab and why each stage of the process is so important. We discuss how embryologists assess egg and sperm quality, what makes a strong embryo, and how technology is improving IVF success rates. Whether you’re just starting your fertility journey or in the middle of an IVF cycle, this conversation will give you the knowledge and confidence to navigate the process.
In this episode, we cover:
- What happens during egg retrieval and fertilization
- How embryologists evaluate embryo quality
- The role of ICSI (intracytoplasmic sperm injection) in IVF
- How technology, like time-lapse imaging, is improving embryo selection
- Common misconceptions about IVF success rates
- Tips for patients going through IVF
Resources:
Find Dr. Aimee’s Fertility Essentials & Supplements


Transcript:
Dr. Aimee: Welcome, Salu! I’m really excited about tonight’s show. The reason is because I have The Embryo Whisperer here. You may not know it, but Salu is an awesome embryologist. He’s actually thawed one of the longest frozen embryos in US history. It was thawed after over 19 years.
Salu Ribeiro: One of them. I have worked with many embryos, have created many embryos.
Dr. Aimee: We’re talking like 5,000.
Salu Ribeiro: 5,000 injections. Yes, it’s a lot of embryos created.
Dr. Aimee: That’s a lot of eggs and a lot of sperm.
Salu Ribeiro: It sure is. It’s wonderful. I’m very glad to be here today. Thank you for the invite.
Dr. Aimee: Of course.
Salu Ribeiro: It’s very exciting to share my knowledge and information with all of you.
Dr. Aimee: You went to UC Davis. What made you say, “I want to be an embryologist.”
Salu Ribeiro: It was a funny pathway. Before, I was going to do computer work and I was going to work doing programming and being a tech in San Francisco. All of a sudden, I got a job on campus, and I started working at the health center. Then one day this nurse said to me, “Why don’t you go into phlebotomy? It’s a good job. You can do that during the weekend, when you’re studying. It’s wonderful.”
So, I did that, and at the same time, I worked on the weekends in a fertility clinic and went to Davis. Eventually, I chose a major because it was time, and I did bio-tech, which is kind of biology with informatics. But I really was intrigued by the fertility world, working at this fertility clinic. Then I finished college and I was invited to work at the fertility clinic as an embryologist. Since then, I just love what I do.
Dr. Aimee: You’re kind of like an embryo whisperer. For other people out there who are perhaps interested in a career in embryology, how many years would it take someone, let’s say from graduating high school until when you’re actually sitting in a lab and working with eggs and sperm?
Salu Ribeiro: Most of us come from the animal world, we do a degree in biology with cell biology and animal biology, or something related to the biology field. Then there are some colleges in the US that offers a major in embryology, but mostly in animal, because you don’t want to be practicing with humans, of course.
Then you graduate, four years, and then you do on the job training at a fertility clinic that will take you. The job training takes about two years. Then there are some master’s programs, which I went to University of Leeds in England, I got a master’s in clinical embryology and andrology to more understand what I do and do some research as well.

Dr. Aimee: And get a whole bunch of degrees.
Salu Ribeiro: Pretty much. One degree after the other. I never thought I was going to have so many degrees after high school. But that’s where I am today.
Dr. Aimee: That’s exciting stuff. We’re going to talk about the nuts and bolts of IVF. I realize we actually look kind of similar, except I have hair.
Salu Ribeiro: And I don’t. Well, that’s how they look at the sperm, they’ll all look the same. We don’t know if they will have hair. We just don’t know, it’s all the same.
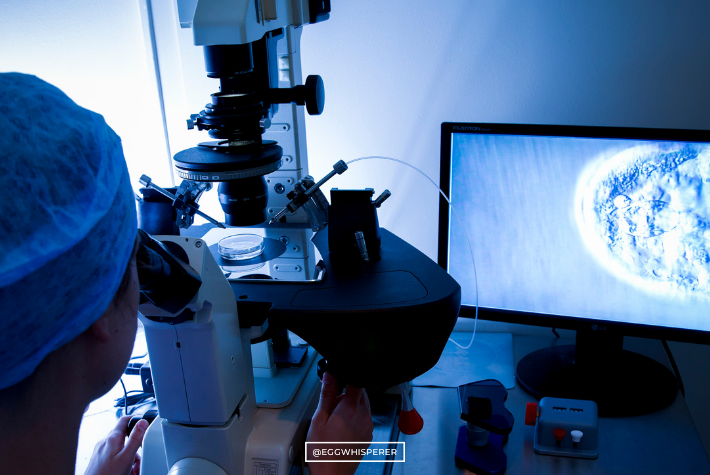
Dr. Aimee: It’s all the same. This is a picture of an IVF lab. This is basically your home.
Salu Ribeiro: That’s my home for eight to nine hours a day. It’s clean air, no sunlight, but nice light. I would say we breathe the cleanest air whatsoever, just like the embryos. It’s a very clean environment.
Dr. Aimee: So, people who are interested in anti-aging therapy maybe should go become embryologists.
Salu Ribeiro: Maybe, yes. No sun exposure.
Dr. Aimee: This morning I did an egg retrieval, I retrieved over 10 eggs from somebody. I put the eggs in test tubes and I hand them to an embryologist like you. Then what do you do from there?
Salu Ribeiro: From there, we dip that into a dish. Test tube babies, because they come from a tube. We dip into a dish. Then we’re looking for eggs into the solution, which is the liquid, and they kind of look like that, the picture you’re showing here. At this point, we don’t know if it’s mature or not, because we cannot assess the maturity. All the cells around, it’s beneficial because that attracts the sperm, that’s naturally attracting the sperm.
Dr. Aimee: What are those cells called?
Salu Ribeiro: Those are the cumulus cells.
Dr. Aimee: Cumulus cells?
Salu Ribeiro: Yes.
Dr. Aimee: You have cumulus cells there. You don’t know if the egg is mature or not. What do you do next?
Salu Ribeiro: Depending on what treatment your physician chooses, whether it’s going to be IVF or ICSI. If they choose ICSI, we have to strip the eggs.
Dr. Aimee: So, there’s a lot of stuff that goes on behind the scenes in the IVF lab.

Salu Ribeiro: Yes, we’re stripping to assess the maturity of the oocyte, which is the egg.
Dr. Aimee: Here we go. Mature or immature? Go…
Salu Ribeiro: That’s immature. You can see the GV, which is the germinal vesicle, which is an immature egg. When they tell you it’s an immature egg, most likely it’s an M1 or a GV.
Dr. Aimee: Okay. Sperm and M1s or GVs don’t like each other. Why?
Salu Ribeiro: They don’t like each other because there’s too much chromosome involved in that environment. Naturally, the human body and nature is amazing to say that’s not good because there’s too much DNA there, so we’ll not fertilize.
Dr. Aimee: Got it. So, GV, M1, not as good.
Salu Ribeiro: Even if I tried to put a sperm inside of this egg, most likely the egg will die or become atretic or not fertilize.
Dr. Aimee: How about this; what if you get an M1 (and we’ll talk about M2 in a second), what if it becomes an M2 like two or three hours later?
Salu Ribeiro: Then there could be a chance that it can fertilize and develop into a normal embryo. But again, there are lower chances to develop into a normal embryo.
Dr. Aimee: What do we call that, something like M1 conversion?
Salu Ribeiro: M1 conversion into M2. We put a note there that the polar body extruded. The polar body is this little guy right there. That’s a polar body that got extruded and that now is an M2.
Dr. Aimee: M2 makes you very happy, right?
Salu Ribeiro: Yes. They make all the embryologists very happy because that’s an egg ready to be fertilized. That’s a golden egg, that’s a beautiful oocyte.
Dr. Aimee: Yes. When you look at an egg, you just said that’s a beautiful egg. What about this egg makes it beautiful?
Salu Ribeiro: You can see that the oocyte is not dark or granular, it’s a very smooth surface of the oocyte. The PV space is not that large. The PV space is what it’s called between this space right here, the egg and the zona pellucida. Those are characteristics that we’re looking at to determine if it’s a good quality oocyte.
Dr. Aimee: Got it. I’m going to put up some pictures. This is an egg with vacuoles. What happens when you see this? How often do you see eggs that have vacuoles in them?
Salu Ribeiro: We see them once in a while. Those are signs that they’re not good now. When we inject them, if they’re an immature egg we always inject them with a sperm, and if they develop, good, if not, then it could be a characteristic of the vacuoles.
Dr. Aimee: Got it. So, it doesn’t necessarily mean that you’ll have bad embryos.
Salu Ribeiro: Not necessarily.
Dr. Aimee: But it could be a sign that you may not get as many as you expected.
Salu Ribeiro: Correct. I have seen a patient when four or five were like this and I injected them, I remember even writing the notes, poor egg, and the next day all of those vacuoles were gone and there was normal fertilization. I was like wow, a miracle right there.
Dr. Aimee: That’s awesome. Let’s say you’re an egg freezing patient and you have eggs like this. I know you don’t have eggs, but if you did, knowing what you know, would you consider going through more cycles?
Salu Ribeiro: Definitely. We as embryologists record that information if we see that it’s not a normal looking oocyte, so the physician can recommend another treatment, definitely.
Dr. Aimee: Right. Very good. This is another egg physical characteristic that is sometimes seen. It’s grainy. Tell me about it.
Salu Ribeiro: You can see it’s a little bit grainy here on the top. Those are characteristics that we record when we see them after stripping those eggs.
Dr. Aimee: No one wants to have their eggs described as vacuolated, grainy, brown.
Salu Ribeiro: No, but it’s good information to provide. It’s always better to know the information than not know any information.
Dr. Aimee: Is there anything we can do as human beings that could change the quality of the eggs? Or maybe this is even a better question. Is there something about the lab environment that can cause this?
Salu Ribeiro: All of the lab environments in the Bay Area and in the US are pretty good, they are regulated by CAP and those are good institutions. I would say those labs are great, they provide good services. Sometimes just the egg quality is affected. Probably the patient went through some problem in the past, health habits, smoking, anything that neglects your health could affect your oocyte quality.
Dr. Aimee: Right. I tell patients to get into the best shape of their lives, consider supplements, acupuncture. Anything and everything you can do to improve egg quality, do it. It doesn’t necessarily mean that it’s going to work, but it can only help.
Salu Ribeiro: Absolutely.
Dr. Aimee: Tell me about what you see in this picture here.
Salu Ribeiro: This is an oocyte, or even a blast with all those fragmentations. They’re more in the 50% fragmented oocyte. That’s a pretty poor quality oocyte, definitely.
Dr. Aimee: If you saw this, would you even try to inject it with sperm, or is it just not a mature enough egg to do that?
Salu Ribeiro: The criteria is if you see a polar body and it’s not an awful egg, then definitely you want to inject because you always want to give a chance.
Dr. Aimee: I love that.
Salu Ribeiro: There’s never a never in the lab. There’s always a possibility. I believe there’s always a chance. I’ve seen embryos that came from death and survived. It’s amazing what we see.
Dr. Aimee: It is amazing. What about this egg?
Salu Ribeiro: This egg is a little bit fragmented polar body. It looks like you have two or three right here. That is just a fragmented polar body. That’s something that you want to note if you see many of them.
Dr. Aimee: How does that happen?
Salu Ribeiro: That can happen through the process of when you’re stripping them, or it also could be that when it got retrieved, the pressure. There are many questions that it’s unknown. It could be just that it was made like this.
Dr. Aimee: When you see an egg like that, you typically don’t see 10 like that, right?
Salu Ribeiro: No, it’s just one. Between the cohort, you see one or two, or none. It depends.
Dr. Aimee: Would you still inject?
Salu Ribeiro: You still inject, definitely. That’s just a normal M2, just with a polar body that’s fragmented.
Paula: There’s a question.
Dr. Aimee: Yes. What’s the question?
Join The IVF ClassPaula: In a regular IVF cycle without ICSI, is it normal procedure to strip the eggs before allowing the sperm to naturally try to fertilize the egg?
Dr. Aimee: Basically, is it normal to do IVF or ICSI and how do you choose?
Salu Ribeiro: The choice is based on the SRM guidelines where they recommend IVF unless if you have poor sperm quality. It’s best to just ask your doctor. She or he will be able to determine what’s the best treatment for you.
Dr. Aimee: Right. I’m going to ask you this other question now that we’re segueing into sperm. The question is do you actually prefer ICSI if a patient is doing genetic testing?
Salu Ribeiro: That’s a great question that a lot of people have asked. The best answer that I got from a genetic counselor that spoke directly with the reference lab is it does not matter if you’re doing PGS if you do ICSI or IVF.
Dr. Aimee: Technically, what do you prefer? What makes your life easier as an embryologist as far as technically speaking?
Salu Ribeiro: There’s no preference for myself. When you’re removing the trophectoderm, you don’t want to put combined DNA of the sperm with the trophectoderm. By the time that you do the trophectoderm biopsy, the embryo probably already fell off and you have no problems with contamination.
Dr. Aimee: Got it. For those of you who don’t know what a trophectoderm is, or a trophectoderm biopsy, keep watching because we’re going to get to those terms in a second.
Let’s talk about swimmers. Do swimmers really matter? That was a question that I got by email. Does the sperm integrity, strength, health matter when it comes to fertilizing eggs?

Salu Ribeiro: Yes, it definitely does. I have presented myself a case where we used the same egg donor.
Dr. Aimee: So, you have one set of eggs.
Salu Ribeiro: From that cohort she had 20 eggs; 10 went to sperm A and 10 went to sperm B. Sperm A was very poor quality, poor morphology, poor motility, poor count or lower count. Overall, that sperm quality was pretty poor. Therefore, the embryo quality from that case was developed very poor.
Dr. Aimee: How many embryos did they end up getting in that batch?
Salu Ribeiro: I think it was only one.
Dr. Aimee: Got it. So, then B…
Salu Ribeiro: B was great sperm, super swimming, they were great. They met a two-fifth standard.
Dr. Aimee: What does that mean, two-fifth standard?
Salu Ribeiro: We use a guideline through WHO, the World Health Organization, and they set numbers for us to say what’s normal and what’s not normal, because we need to decide what’s normal and not normal based on that table. That patient had wonderful sperm, met all the standards according to WHO, and those embryos developed into beautiful blastocysts. I think she had five or six frozen. It was a great case.
Dr. Aimee: I think that’s such a great example that you talk about tonight, because so many of us as women just internalize everything and blame ourselves and think it’s us.
Salu Ribeiro: It’s not always the woman or always the man, it’s 50/50.
Dr. Aimee: Yes. Salu and I could talk about this all day, every day, for hours and hours. And we do. This is super fun for us. Thank you again for being here.
Salu Ribeiro: Of course.
Dr. Aimee: You have the egg and now we have to inject the egg with sperm. Tell me what’s going on in this slide.
Salu Ribeiro: That’s the ICSI, which I can see right here.
Dr. Aimee: What does that stand for, ICSI?
Salu Ribeiro: Intracytoplasmic sperm injection.
Dr. Aimee: Got it.
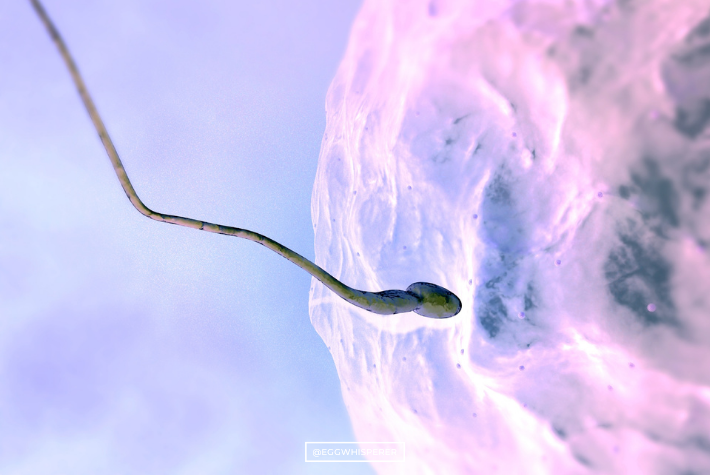
Salu Ribeiro: That’s when you get a very thin needle, right here, with another holding needle, and you will then place in one sperm inside of that mature oocyte. One to one. People sometimes ask, “Do you put two sperm for two kids or how are there twins?” No. We put one sperm into one egg. If that egg divides and then divides and one of the cells hatches out and the other one becomes, there’s a chance that both of those cells from the same egg and the same sperm becomes twins.
Dr. Aimee: Right. Very rarely, though. That’s super rare.
Salu Ribeiro: Yes. But that’s the case where it’s only one and one.
Dr. Aimee: I get that question, too. I thought I was the only one where people would say, “Can you put two sperm cells in the egg so I can have twins?” I don’t know where that comes from. Maybe you know the same people.
Salu Ribeiro: Here’s the holding. We’re holding the egg. We’re not harming the egg. Just remember, think about if you have an egg and you’re holding under a solution under a drop under the microscope in a controlled environment where the temperature is always warm.
Dr. Aimee: That sounds very relaxing.
Salu Ribeiro: It is very relaxing. ICSI can be very relaxing. It’s kind of therapeutic sometimes, because you’re just looking at them and listening to music.
Dr. Aimee: What’s your song of choice?
Salu Ribeiro: That’s a good question, because we rotate, we have Pandora in the lab. Depending on who arrives first in the morning, that person chooses the music. So, we have all kinds of music.
Dr. Aimee: I see. Let’s say 20 mature eggs. How long would it take you to inject them?
Salu Ribeiro: It takes about two minutes per egg, a minute and a half. You pick the sperm, put it inside the egg. Sperm selection, did we talk about that?
Dr. Aimee: Oh. I want to talk about it. Let’s talk about it.
Salu Ribeiro: Okay. Sperm selection is another factor. How do you choose what’s the best sperm? The best sperm that you want to choose is the one with the best swimming, so you want them to be swimming very quickly.
Also, you want them to have a morphology. What’s the morphology of nice sperm? You don’t have two tails, you want to have only one tail. You want it to only have one head. Sometimes, when you see the sample, there’s two heads, three tails, they look like octopus.
Dr. Aimee: You don’t want octopus sperm.
Salu Ribeiro: Right. Then you place that inside of the egg. The next day you’ll look for fertilization.
Dr. Aimee: There’s something that a lot of people are doing now called PICSI. I think of it as picking the best sperm for ICSI. Tell me how that works.
Salu Ribeiro: The PICSI method is when you will choose a mature sperm that binds to that plate.
Dr. Aimee: Is this the plate or is this a droplet here?
Salu Ribeiro: That’s the drop in the plate.
Dr. Aimee: Got it.
Salu Ribeiro: They bind. The tiny little things there are the sperm. They bind to that plate because they have the receptor, the plate and the sperm had, that they are fully mature. We look for full maturity and also for best morphology when they bind to the plate.
Dr. Aimee: So, the ones that have bound tend to be more genetically normal.
Salu Ribeiro: Correct. You will then select that and then inject into the egg, just like ICSI.
Dr. Aimee: Why doesn’t everyone do it?
Salu Ribeiro: There’s a lot of steps that you have to do. You have to use a special plate. It takes time. You have some sperm that bind to the plate that are not morphologically normal. Also, you want to have a nice sample. If you have too few sperm, they will not bind.
Dr. Aimee: You still need enough sperm to be able to do this.
Salu Ribeiro: Correct. You have to meet specific criteria to fit into the category of the study that they developed.
Dr. Aimee: Got it. Now I want to talk about you’ve made the embryo. You’ve injected the sperm into the egg, and then what happens? How do they grow?
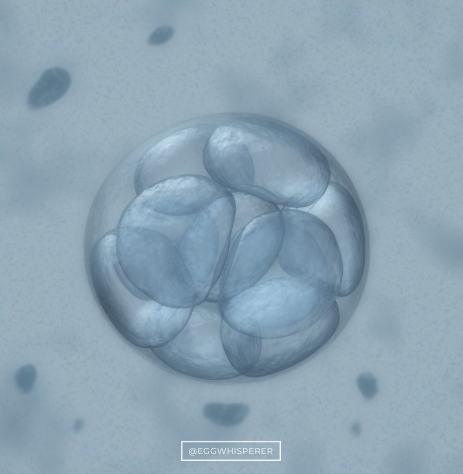
Salu Ribeiro: They start dividing. They divide between two cells, as you can see, four cells, eight cells, they become a morula, they become a blastocyst. Those are the days that we call in the lab. A day two embryo, most likely you’ll be seeing that on day two. Day four and day three embryo, you see four cells to eight cells. When I say cells, what are cells? Cells are things that you can count inside. Those are blastomeres. You can see one, two, three, four. Then also we assess for fragmentation.
Dr. Aimee: How pretty the embryo is.
Salu Ribeiro: Correct. Fragmentation, if those blastomeres, those cells, start degenerating or… think about Dipping Dots ice cream.
Dr. Aimee: I love that ice cream.
Salu Ribeiro: I don’t want to see Dipping Dots ice cream in there. Those little dots are fragmenting embryos. Those are nice grade one assessment fragmentation one, symmetry one as well, so those are great embryos.
Dr. Aimee: The degree of fragmentation and symmetry is related to the chance that the embryo is going to be genetically normal, stick and grow, and turn into a healthy pregnancy. Right?
Salu Ribeiro: Developed a nice blastocyst, correct. If they are poor quality on day three, they’ll most likely arrest as they grow in the lab.
Dr. Aimee: When you say arrest, does that mean they just stop growing?
Salu Ribeiro: They stop growing.
Dr. Aimee: Arrest, no further cleavage, degenerate, they’re just not viable anymore.
Salu Ribeiro: They’re not viable anymore.
Dr. Aimee: You can actually see it. You can actually tell when you’re looking at the cells that they’ve stopped growing.
Salu Ribeiro: Because you see on day five, for example. If you see on day five and you start seeing this on day five, those are arrested embryos, they will not further develop into blastocysts.
Dr. Aimee: When we say day three and day five, what that means is three days after the egg extraction or the egg retrieval procedure.
Salu Ribeiro: We call the day of the retrieval day zero. Day one is the fertilization. Day two, day three, day four, day five, up to day seven.
Dr. Aimee: So, chickens. What do chickens have in common with humans? It’s like a 2AA embryo right there.
Salu Ribeiro: Yes, because you can see a little bit of the ICM. What are those shells? Those shells are called the zona pellucida. They hatch out just like a chick did there. I was an embryo, I looked like that. I don’t know if I was a 5AA or a 5AB. I think I was 5AA. Both of us were 5AAs.
Dr. Aimee: Both of us. I was a 6AA on day five. That’s what my mother tells me.
Salu Ribeiro: So, it shows an advanced embryo.
Dr. Aimee: Very advanced.
Salu Ribeiro: Those are embryos that you most likely are looking at day five, day six, or day seven. Those are blastocysts. They’re hatching out, so you see the trophectoderm. Trophectoderm is the future placenta which will attach to the epiphyllum of the uterus and will become the placenta. The ICM, which is right here, the darker part which is a glob of cells. Those are the ICM, the inner cell mass. That’s the future fetus, the future baby.
Dr. Aimee: Right. That’s the first letter score that an embryo gets. The first number one through six refers to how expanded or hatched the embryo is. Then you hear terms like expanded blast, partially expanded blast, fully hatched, all those kinds of things.
Salu Ribeiro: Those are hatching blasts, so I would call that a 5-something, 5AA or 5AB.
Dr. Aimee: And then the second letter refers to the trophectoderm quality.
Salu Ribeiro: The quality of the trophectoderm, so it’s how many cells you see there. Sometimes we call them C. Sometimes it’s like I had a C embryo that was not frozen, and people say, “Why didn’t you freeze my embryo?” It’s because most likely those cells would not survive a freezing and thawing process and they’re not viable to attach.
Dr. Aimee: They’re not really good enough quality to turn into a healthy pregnancy.
Salu Ribeiro: Correct. They will not attach, and if they attach, they could cause miscarriage or other things that you don’t want to happen.
Dr. Aimee: Yes. For us, if an embryo had the chance to stick and grow, certainly we would give it that chance even if it was like a 1% chance. But if the embryo already shows signs that it’s not alive or viable, we’re not going to freeze it and we would strongly consider against transferring it.
Then another term that people talk about is assisted hatching. When do you do that in the process?
Salu Ribeiro: Assisted hatching is recommended based on certain population. It can help with implantation. Patients age, FSH, if the embryo or egg was frozen before, because during the freezing process the zona pellucida, which is the shell, can become hard and it does not expand. You want that to expand to hatch out.
Dr. Aimee: Then when is it done? This is a day three embryo.
Salu Ribeiro: That’s a day three embryo, that’s done. When you’re looking at those embryos, if you’re doing PGS or if you’re doing a transfer, assisted hatching is recommended. The question is how do we do it? There are different methods in the market that people do. There’s mechanical, there’s chemical.
Dr. Aimee: Mechanical is with a needle.
Salu Ribeiro: Correct. You just hatch with a needle. The chemical is when you put an acid near the zona pellucida and it will dissolve the zona pellucida. Most IVF clinics in the US will use the laser method with a precise laser that hatches.
Dr. Aimee: You can see that right there.
Salu Ribeiro: Right there, so there is a little hole in the zona pellucida.
Dr. Aimee: Is there ever a time that you would not hatch a day three embryo if you were doing PGS?
Salu Ribeiro: No. Most of the practices we all hatch on day three for PGS, because we’ll facilitate the herniation of the trophectoderm.
Paula: There’s a question. What about PCOS patients, do they have assisted hatching?
Dr. Aimee: As far as assisted hatching, yes. I don’t discriminate against patients. It’s not like I discriminate against the embryo and say no assisted hatching for you because you have PCOS. I would say most of my patients still take the opportunity to do genetic testing, so we would definitely do assisted hatching. Having PCOS wouldn’t prevent you from benefitting from that.
Salu Ribeiro: It’s a good question.
Paula: Thank you.
Dr. Aimee: So, now it’s the biopsy. That sounds really scary. I think of I would want someone operating on my baby-to-be who has no tremor. I notice when you were doing all of the stuff with your hands up here that you don’t shake. No shaking. How important is it for you to be totally still and be really good at this procedure?
Salu Ribeiro: The benefit, because you’re using micro manipulators, again, as you explained I was very good about my hand coordination. Every movement that you do with those joysticks, when you’re controlling the holding or the biopsy needle, they are magnified by your movements. You will hold this, one hand with your holding pad, and the other one you hold the herniation of the trophectoderm. Then you push it a little bit, very gentle because you don’t want to destroy the embryo.
Dr. Aimee: Could you, could someone destroy it? If you had the person who was answering the phone at the front desk and all of a sudden you were like, “Hey, go pretend you know how to do embryology.”
Salu Ribeiro: It takes a lot of years and a lot of manipulation for you to be able to do it.
Dr. Aimee: So, a lot of practice before they put you in charge of biopsies of people’s precious embryos.
Salu Ribeiro: You end up doing a lot of practice with research embryos.
Dr. Aimee: That totally makes sense. We talked about embryo biopsy and now PGS. What does that stand for?
Salu Ribeiro: PGS is preimplantation genetic testing, or I call it PGT because the T is for the Testing. We define two categories, the screening, which is PGS, and PGD, which is diagnosis. The PGS is when you’re screening for all of the chromosomes in the embryo. That’s very important because you want to make sure that you have all of the chromosomes from your mom and from your dad. If you’re missing any or having too much chromosome in there, that could be a problem.
Dr. Aimee: Right. It could cause implantation failure, recurrent pregnancy loss.
Salu Ribeiro: Then the PGD is when you’re diagnosing the embryo. Think about a prenatal for embryo. That’s when you’re doing a diagnosis for a specific gene. Perhaps you have hemophilia in your family or sickle cell, any genetic disorder that you want to eliminate from your family. Just keep in mind, we don’t remove the disease from the embryo. We just check to see if the embryo has it. From the pool that we have, we check it. We cannot edit an embryo.
Dr. Aimee: Right. You can’t create a designer baby. You can’t make a brown-eyed baby blue-eyed or a short baby tall or you can’t make them blonde.
Salu Ribeiro: There’s no such technology yet for that.
Dr. Aimee: Do you really think it’s going to come?
Salu Ribeiro: Like PGS, we thought that was not there because now people are doing family balancing.
Dr. Aimee: Gender selection, basically.
Salu Ribeiro: Gender selection, yes. That’s something that we never thought was going to happen, but… I don’t see that as a case. People are not choosing gender. They just want a healthy baby, that’s all. Most patients don’t do gender selection. It’s something that we’re worried has an ethical part, but I don’t see that nowadays.
Dr. Aimee: Now that you’ve done the biopsy, now you have to freeze the embryo because you have to wait for the genetic testing results to come back. There’s so much stuff you read online from studies that frozen is better than fresh. How do you actually freeze an embryo, what does that process involve?
Salu Ribeiro: That’s a great question. I’ll explain it in very simple terms. Think about if you put your embryo into a sugar solution drop.
Dr. Aimee: That sounds nice.
Salu Ribeiro: Then all the water will come out of this embryo. Then you dip the embryo into liquid nitrogen. It’s a very simple method where you just remove all of the water out of the embryo, because the water causes ice crystal formation and that will rupture the cell and damage it.
Dr. Aimee: That doesn’t sound good. So, you do it in a safe way. You don’t lose embryos from freezing.
Salu Ribeiro: We don’t, because we can see the embryo when we load into the pie pad. They’re small, but we’re looking under the microscope and we can definitely see the embryo being set there. It’s a very sticky solution, so we can see the embryo is stuck there. We dip it into the nitrogen and then it’s frozen.
Dr. Aimee: How long would it take you to freeze five embryos for somebody?
Salu Ribeiro: Each embryo takes about three minutes.
Dr. Aimee: Total process for you, you’re just like, “I’m going to go freeze an embryo,” and three minutes later that embryo is frozen?
Salu Ribeiro: Yes. That’s pretty much it. Two minutes plus one, and you’re done.
Dr. Aimee: I’m sure there’s a whole logging process, too, of patient name and labeling.
Salu Ribeiro: Yes.
Dr. Aimee: So, it’s not just three minutes.
Salu Ribeiro: Three to five.
Dr. Aimee: You’re just fast.
Salu Ribeiro: It’s just a very simple process. You log into the patient’s record, you put that you froze the embryo, you print your labels, put the labels on the stick. A lot of people are like, “Don’t you mess up the embryos?”
Dr. Aimee: I tell them no, never.
Salu Ribeiro: Never.
Dr. Aimee: Never, ever, ever.
Salu Ribeiro: We always have two people look at the ID of the patient before we even touch the freezing method.
Dr. Aimee: To make sure that you’re getting the right embryo. Same with sperm, same with eggs, same with everything.
Salu Ribeiro: Correct. We always have two embryologists. Any process in the lab, every time that you touch, you have another embryologist with you to make sure that you have the right patient.
Dr. Aimee: Scenario; there’s an earthquake in the Bay Area. What’s going to happen with all of those embryos in the tank?
Salu Ribeiro: That’s a good question. The good thing is that the embryo storage does not require energy, it doesn’t require power. It’s liquid nitrogen. There’s liquid nitrogen inside of this tank, as you can see here. The only concern is to have the people who deliver the liquid nitrogen available to fill up those tanks.
Dr. Aimee: How many times a week do they come to deliver liquid nitrogen?

Salu Ribeiro: Depending on the size of the tank, there are many variables that you want to take into account. A tank this size behind me, and if you don’t open it daily, that can stay fine for five to seven days.
Dr. Aimee: Is it your job, or do you guys rotate whose job it is to load and pour?
Salu Ribeiro: It’s an automated filling. This one is an older tank. The newer tanks nowadays have an automated filling, so it fills automatically. When you reach the level, it stops. It’s connected to my phone, the alarm system, so I will get notifications if the tank is low, if the incubator is alarming. Anything that happens inside of the lab, I’m notified on my phone within seconds.
Dr. Aimee: What about a power outage? That wouldn’t hurt the embryos, right?
Salu Ribeiro: That will not hurt them. But the incubators are connected to the power source. A lot of people ask those questions.
Dr. Aimee: But there are multiple levels of protections, like generators.
Salu Ribeiro: There’s a generator, there’s a UPS battery connected to the incubators, so there are many levels of security and protocols in place. We’re in the Bay Area, we’re connected to all of the fertility clinics. In case of emergency, I can transfer the embryos from my facility to another facility so that they can take care of those babies, those embryos. It’s a great method.
Dr. Aimee: Now it’s transfer day.
Salu Ribeiro: Transfer day is a big day.
Dr. Aimee: You’re in charge. You have such a huge role in these people’s lives and they don’t even know who you are. It’s just nuts.
Salu Ribeiro: I just appear in the room.
Dr. Aimee: You just appear in the room and then you disappear, it’s like two minutes. What do you do with the embryo?
Salu Ribeiro: We’ll load that embryo into the catheter and give it to the physician for the transfer. In the morning, we look at those embryos, we give the grading to the physicians. Between the physician and the patient, they’ll discuss how many they’ll be transferring. They select one, they’ll let us know, and then we’ll place that into a transfer dish and be ready for the transfer time.
Dr. Aimee: Right. Patients get a picture of their embryo, sometimes they can see it on the screen.
Salu Ribeiro: Yes. We take a picture of those embryos. They can see the name of the patient on the dish that I’m loading the embryo from. Everything has a chain of custody.
Dr. Aimee: Nice. When you do a transfer, I call it the spark of life, where you push the end of the syringe and then you see this beautiful white flash. What is that? The embryo is supposedly microscopic. What is it that we’re actually seeing?
Salu Ribeiro: We’re seeing the air bubble that reflects on ultrasound. That’s an assurement. Where I do the transfer, we put two little bubbles, so the embryo is between the two little bubbles. You can see if the embryo got transferred.
Dr. Aimee: When you say bubbles, like you’re blowing bubbles or where are the bubbles coming from?
Salu Ribeiro: It’s an air bubble that is created manually on the catheter. Also, we double check. We bring the catheter back and people say, “What are they doing back in the lab with my catheter?” We take the catheter back into the lab and make sure, because the embryo can get stuck sometimes to the tip of the catheter or it doesn’t get loaded completely. Then we can reload, put it back, and your chances are the same.
Dr. Aimee: Basically, you can have a sticky embryo.
Salu Ribeiro: Just sticky.
Dr. Aimee: It doesn’t mean anything. You just load it back up and put it back?
Salu Ribeiro: Just put it back in.
Dr. Aimee: Got it. Okay. Cool.
Paula: We have a question from Facebook. Is it easier to freeze embryos rather than eggs?
Salu Ribeiro: ASRM just removed the research criteria for egg freezing. Think about us humans, we’re big cells, we’re a lot of cells. Even freezing a whole body is not possible right now.
Dr. Aimee: Well, it is, but it’s expensive.
Salu Ribeiro: Well, you can freeze it, but what’s the success rate of thawing you?
Dr. Aimee: Zero.
Salu Ribeiro: We don’t know yet. Same thing. The embryo is many cells. An egg is just one cell. It’s just a bigger cell.
Dr. Aimee: But you’re really good at it. If you froze an egg, the survival rate is close to 100%.
Salu Ribeiro: Yes. It’s just great. That’s why Facebook, Google, and all those tech companies are encouraging their employees to freeze their eggs.
Dr. Aimee: Right.
Salu Ribeiro: Who is the Egg Whisperer? You want to see Dr. Aimee. I told my sisters, “Once you’re ready to have a baby, if you want to freeze your eggs, you come and talk to Dr. Aimee.”
Dr. Aimee: Basically, when I have those conversations with patients it really has to do with the FSH level, the AMH level, what the family size goal is, would you consider doing it within five years, it meaning being a single mom by choice, or would you want to wait for a partner. Those are all the parts of the conversation that I have with patients before deciding on whether you create embryos upfront or just freeze eggs. There’s a lot involved, for sure.
Salu Ribeiro: I’ve even had some cases I’ve seen where a patient went through egg freezing by herself and then she created embryos as well, just to have an option Plan A and Plan B.
Dr. Aimee: Absolutely. That’s a great way of doing things, too.
There’s a lot of stuff trending out there right now. I’ve received an article, it’s on my Facebook professional page, from The Cut about how patients are potentially wasting embryos that could turn into healthy pregnancies, thinking that they’re actually abnormal from PGS when they really could result in a healthy pregnancy. I call that the murky crystal ball of IVF medicine.
So, I just wanted to talk a little bit about this word, mosaicism, aneuploid, and euploid, and what that actually means. Does anyone actually transfer abnormal embryos, the embryos that have an abnormal chromosome?
Salu Ribeiro: I have not seen a case yet. But some physicians are recommending to their patients not to discard them just yet, because of new technology. Fertility treatments since our first IVF baby, she was born 1970-something.
Dr. Aimee: I don’t know, but she just had a baby.
Salu Ribeiro: Yes, she had just a baby. So, it’s a brand new technology still, and there’s a lot to learn. I believe that mosaicism, euploid, and aneuploid is still a field that we need to learn more.
Dr. Aimee: If you’re a patient of mine, I want you to talk to me about your concerns. All of my patients will get a report, and that genetic testing report will tell you which embryos are normal, which are not, and which are what we call mosaic. Depending on the chromosomes that are abnormal, there may be an opportunity to transfer, but it certainly doesn’t mean that everyone should consider it and every embryo is a candidate for transfer.
This article has created lots of panic out there. I can tell you it’s just trending, and people are texting, emailing, Facebook messaging it to me, and I definitely saw it as soon as it came out.
Salu Ribeiro: I would say I don’t talk mainly with patients, but friends that ask my opinion, I always tell them just talk to their physician and they’ll have the best answer for them in that specific report.
Dr. Aimee: Right. I just wanted to say thank you, Salu, for being here tonight. I know we still have a lot of questions. I know there are a couple of questions that we had emailed.
One of the emailed questions that I got was, “I’m 37 years old, I’ve been trying for eight years. Is IVF good for me?” What I would tell that person, because I don’t know them, is you really have to figure out what’s going on, what’s wrong. You can’t just go into IVF if, let’s say, there’s no sperm. You wouldn’t want to have that kind of surprise. Make sure that you understand what your fertility diagnosis is before you do IVF and do whatever you can to make things as good as possible.
We used to say IVF is the most comprehensive fertility diagnostic test, it’s only through IVF that you actually know what the egg and sperm will do together. But now we have fertility genetic tests that can guide you a little bit better before you do IVF, that can teach you more about embryo development, like looking at DNA fragmentation of sperm and epigenetic changes in sperm and fertility gene tests in women.
All of these things together can guide you, so you don’t do an IVF cycle and say, “Oh my god, why did this happen?” At least you go into it saying, “I was kind of expecting or I knew that there was a chance that could happen. I’m really happy that there’s one high quality embryo.” Rather than looking at your cycle and be disappointed, be happy with what you have.
That’s what I would tell the 37-year-old who has been trying for eight years.
Another question that I was asked was about brown grainy eggs. I think we kind of answered that.
Salu Ribeiro: It’s just the quality of the oocyte or the embryo.
Dr. Aimee: Yes. Another really important question that a lot of people are asking, because patients who have done IVF two or three years ago, had embryos frozen and now they’re asking is it safe to genetically test those embryos. I have one more question that I was asked, too, after that. Is it? If you have a set of eight high quality frozen embryos on day five, would you be comfortable as an embryologist thawing, biopsying, and refreezing them?
Salu Ribeiro: Yes. We have done that quite a few times. That’s a new process. We just thaw them, biopsy them, freeze them, receive the testing and then thaw the ones that are euploid.
Dr. Aimee: For transfer. That sounds like a lot to put a little embryo through.
Salu Ribeiro: It’s very stressful for the embryo, but it’s done.
Dr. Aimee: When you say it’s stressful, do you think it hurts the chances?
Salu Ribeiro: Not the chances. But the thawing and freezing, that process, the manipulation, your embryo is outside of the best environment, which is the uterus, you put it again back in the lab. Not that the lab is a bad environment, but the optimal environment for your embryo is the uterus.
Dr. Aimee: Got it. You’re saying because there are human beings involved, sometimes things happen.
Salu Ribeiro: Patients sometimes request transfer from one embryo to another clinic. The transportation, too, you want to minimize the chances of something happening.
Dr. Aimee: But the chances of something bad happening is pretty low.
Salu Ribeiro: It is pretty low. It’s very low, but there is a chance. If that’s your only embryos that you have, you have to think very much about it.
Dr. Aimee: Right. What about repeat biopsies? We talked about mosaicism or abnormal embryos and should you consider transferring them. What if an embryo has been biopsied once, should you repeat the biopsy? What’s the safety on that?
Salu Ribeiro: The recommendation from the reference lab, they recommend you not to re-biopsy the embryo. Again, some people do it.
Dr. Aimee: Some people do it, and they’ve had live births from it.
Salu Ribeiro: Definitely. It’s just a recommendation.
Dr. Aimee: Okay. Another question?
Paula: Can an egg be tested to see if it has a normal number of chromosomes?
Dr. Aimee: I wish. I wish you could go to the grocery store, like go to Safeway, and be like, “I’m here for my eggs,” and they just take a scanner and beep. Right? Did you invent it, is it coming?
Salu Ribeiro: You can test one egg for chromosomes, polar body biopsy.
Dr. Aimee: But it’s so hard to do.
Salu Ribeiro: It’s a technology that’s not available as much.
Dr. Aimee: And you can damage the egg by doing a polar body biopsy.
Salu Ribeiro: You don’t know what’s the other half, because the other half is the sperm, so you’re only getting certain information. So, no, it’s not enough information.
Dr. Aimee: I wish. I certainly wish that you could. That would make life easy for all of the egg freezing patients out there.
Salu Ribeiro: Even a method that is in development that you, not biopsy, but you can remove the fluid off the blastocele off your embryo and detect for abnormalities.
Dr. Aimee: Right. What you’re saying is there are certain protein markers in the fluid that surround an embryo or egg, and depending on the amount of that marker, that could be a sign that the embryo is normal.
Salu Ribeiro: Yes. It’s a new technology.
Dr. Aimee: Where are with that technology?
Salu Ribeiro: I would say five more years, five to 10 more years.
Dr. Aimee: Hopefully it’s soon.
Salu Ribeiro: Imagine, they have one report that they had an artificial uterus. I imagine I’ll be babysitting babies in the lab.
Dr. Aimee: Sign me up.
Salu Ribeiro: Through science. All that we’ve thought about, all the science fiction movies, it’s happening.
Dr. Aimee: It’s going to happen. You’ll be there and I’ll be here to talk about it. Salu, I really hope that you’re going to come back again. Will you come back?
Salu Ribeiro: Yes, definitely. I will be very happy to do that.
Dr. Aimee: Awesome. We’ll catch Salu again.
Catch more of me and topics like this through The Egg Whisperer Show. Episodes are live-streamed on YouTube, Facebook, Twitter, IGTV and Apple Podcasts. Sign up to get my newsletter. Tune in to The Egg Whisperer Show on YouTube. And sign up for The Egg Whisperer School.